Quantified Self Public Health is back! 150+ health geeks of many stripes will gather on Thursday, May 14, in San Diego to discuss how access to personal data could benefit individuals and society.
It is an invite-only meeting (sorry!) but filled with voracious documentarians like Joyce Lee (read her Storify from last year) and, well, me (read my round-up post, which also links to others’ blogs). Follow the tweets on the #QSPH hashtag, too.
Observations and conclusions from last year’s QSPH event were captured in an in-depth report (PDF) and in a series of videos. Here is one of my favorites: Ian Eslick’s talk on the role of personal experimentation in the medical and scientific process:
This year it will be my privilege to interview Don Norman, a design pioneer, on stage.
To prepare, I’ve been reading sections of his books, The Design of Everyday Things and Emotional Design, and watching talks like this one:
I was struck by three themes of Norman’s approach:
1) Solve the correct problem.
My reaction: Boy, does health care need to grok this point. I can’t wait to ask him how to recognize when you’ve dug deep enough into the roots — and what tools to use to get there.
2) Pleasant, attractive things work better.
Reminds me of Michael Graves’s tart review of his hospital room: “I can’t die here. It’s too ugly.” And then he went on to make hospital rooms more beautiful and functional.
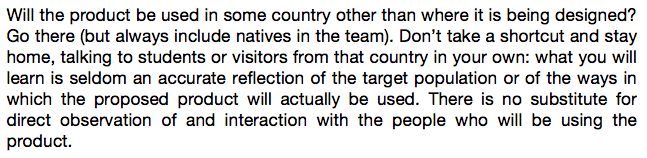
3) There is no substitute for direct observation of and interaction with the people who will be using the product.
Yes! I couldn’t agree more. Participatory research *must* come to health care.
Read the full quote from Chapter 6 of The Design of Everyday Things, and, as a thought experiment, substitute “natives” for “patients”:
This point reminds me of conversations I’ve had with people who design communications for HIV clinical trials. They need to use “one voice with many inflections” — that is, one set of facts, but tailored to the population they are targeting, such as sex workers in Thailand vs. Peru.
Switching gears…
A key element of the QSPH meeting is that it will be populated by toolmakers and tinkerers. People who make and hack their way to insights about health. So I’m also reading Mark Hatch’s book, The Maker Movement Manifesto.
One of my recent obsessions is the health innovation that is happening at home — the hacks, tips, and tricks that regular people invent to make their lives better. Some are simple, like using a baker’s spatula to turn a large person in bed or sticking a pen through a tennis ball so someone with low dexterity can write. Some are more complicated, like the Do-It-Yourself-Pancreas-System or the Auvi-Q epinephrine injector (both created by people living with the conditions being addressed).
How might we harness the energy of all the people who are making a way out of no way, every day, in health care (that is, patients and their loved ones)? How might we empower them with data and resources? How might we learn from them, and them from us?
Please let me know if you have a question for Don Norman. I know our time will go very quickly, but I want to squeeze as much as I can into the conversation!
Yes, please send us your questions.
Don
Don Norman writes in The Design of Everyday Things about the important role of “non-expert knowledge.” Does non-expert knowledge mean “less knowledge” or does it refer to a different kind of knowledge? I’d love to hear you two discuss this.
Great question!! Thank you.
We’re so excited to have you there and participating once again! It was wonderful to have you last year (and since you won’t plug yourself, I will – check out Susannah’s wonderful talk on “data as a mirror” here: https://vimeo.com/95563082).
One of the issues that I hope we discuss at the meeting and that may color your discussion with Don is related to your ideas above, particularly your use of the word “empower” – equity and access. You mentioned that your conversation may help us understand how we can empathize and understand the patient’s perspective. How we can use the strength of Don’s amazing work in human-centered design to impact our own work in research, clinics, and even foundations and institutions. I am left wondering how these principles of design can impact our ideas about how we can tackle the thorny issues of equity and access.
Equity can take on many meanings in many different contexts. Access might pertain to data, care, or even human rights. These are issues that will define our culture now and into the future. Can we use design to not just build great products, but build a great culture?
I’d like to hear more about the role of spirituality (however you chose to define it) in the design of everyday things, but most importantly in the design of health related products. It seems to me that one’s sense of purpose and meaning are largely absent from the healthcare/QS/design conversation.
Natasha, you are singing my song. Ernesto was kind enough to link to my talk from last year when I walked right up to the edge of this topic — not mentioning spirituality, but certainly bringing humanity into the conversation. How might we be gentle as people face the truth about their health? How might we lead them toward a better path — or, better yet, how might they lead US toward a better path?
I would categorize this as a “root” issue. What problem are we REALLY trying to solve when we design health interventions?
Thank you!!!
Patient generated data still aren’t valued in the clinical environment, so why do we bother creating it?
Or, as Nir Eyal asked me, “What problem are my end users REALLY trying to solve?”
From my vantage point, self tracking touches on deeper impulses than merely creating evidence of disease or fitness or adherence.
Much like cracking the egg, the process may be the product.
Won’t you please risk a bit of existentialism in your conversation? 🙂
I agree with Natasha, let’s take that risk. I’m going to be citing the recent IoM report until I’m blue in the face – the one that called out self-reported sense of wellbeing as a clinical metric…
I agree with Natasha, let’s take that risk. I’m going to be citing the recent IoM report until I’m blue in the face – the one that called out self-reported sense of wellbeing as a clinical metric…
Gary, which IOM report are you referencing?
It’s called “Vital Signs: Core Metrics for Health and Health Care Progress”
Just released on April 28, 2015
LINK: https://www.iom.edu/Reports/2015/Vital-Signs-Core-Metrics.aspx